
If you’re reading this, you probably know that I’m obsessed with longevity. But to really understand longevity, you must understand metabolic health, insulin resistance and, by extension, one of its end-results: type 2 diabetes (T2D). Though my medical practice does not focus on type 2 diabetes, I have taken care of several patients with T2D over the past few years. When I was in medical school I was taught many things about T2D, but one stands out most: T2D is incurable, I was told. Once you have it, you’ve always got it, and the best one can do is “manage” it as a chronic—but irreversible—condition.
But is this really true? Asked another way, is T2D reversible?
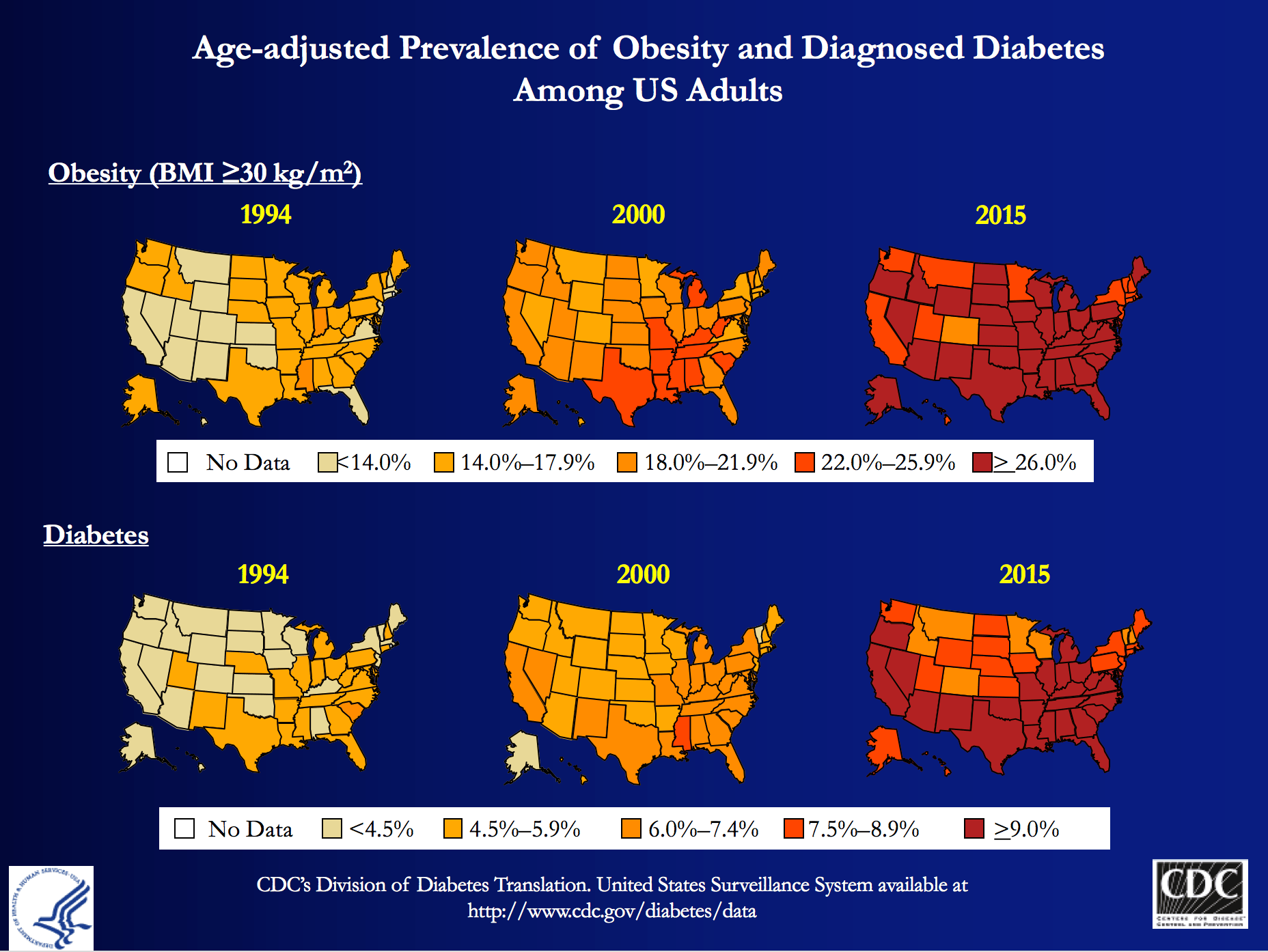
My obsession is partly due to my personal journey to better metabolic health, which I’ve documented elsewhere on this blog, and spoken about publicly. But those facts alone, don’t fully explain why I wanted to be involved with Virta Health (I’ll get to them shortly). T2D is a massive societal problem that has the potential to literally bankrupt countries: More than 29 million Americans have T2D and more than 80 million are pre-diabetic. And whether you view it through the lens of population health, or the lens of an individual patient, T2D is perhaps the biggest healthcare challenge of our generation.
At the population level, T2D costs Americans more than $300 billion per year: one of every three Medicare dollars is spent on T2D, and one of every six healthcare dollars is spent on T2D. At the individual level, patients and payers (employers and insurance companies) spend thousands of dollars (often more than $10,000) in annual expenses for medications and procedures with significant side effects, and much higher risk of developing cardiovascular disease, cancer, Alzheimer’s disease, blindness, amputation and kidney disease.
The traditional approach—which is clearly not working—is to “manage” this chronic condition with medications and the ever-ubiquitous “eat-less-avoid-fat-exercise-more” lifestyle interventions. At best, this approach only slows down the progression of the disease. Furthermore, many diabetes drugs have their own side-effects and diabetes management has a dismal diabetes reversal rate of about 1%. To date, the only clinically proven way to reverse T2D has been bariatric surgery, which is costly and not without risk. If one great thing has come from bariatric surgery, besides the obvious help to those have been successfully treated, it is that any physician or scientist paying attention to the results can’t help but notice that the reversal of T2D in these patients post-operatively seems uncoupled from their weight loss. In other words, adiposity, while correlated with T2D, is not likely the cause.
Every doctor has his (or her) “Patient 0”—the one who really got him (or her) thinking. I’d like to introduce you to mine, RB. When I met RB, he was a 37 year-old Mexican man with a family history of T2D who had a “high” glucose level on a screening blood test. His two-hour oral glucose tolerance test (OGTT) is below.

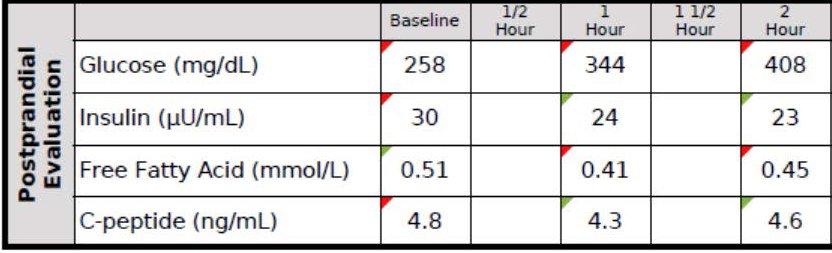
You don’t have to read these for a living to see this isn’t ideal. As you can see, his fasting glucose was 258 mg/dL and his fasting insulin, 30 uU/mL. When given 75 g of glucose, his glucose rose to 344 mg/dL at 60 minutes and 408 mg/dL at 120 minutes, all the while his insulin level fell from 30 to 24 to 23. These numbers alone confirm the diagnosis of T2D. But if we needed more evidence, his HbA1C was 9.7%, corresponding to an average blood glucose of 232 mg/dL (today the diagnosis of T2D is defined by HbA1C >= 6.5%, but I much prefer to use OGTT).
Ordinarily, for a patient with this degree of disease and beta-cell fatigue, I would have opted for at least two drugs, metformin (cheap) and a DPP4 inhibitor (not cheap) and most doctors would have gone straight to insulin, as well. However, due to the patient’s financial circumstances, we opted to only use metformin and dietary modification. The patient worked very long hours in construction and, frankly, was pretty much exercising all day, so there was no way adding more exercise to his day was going to work. If we were going to fix him, it had to be through nutrition. I spoke with one of my mentors, Dr. Naji Torbay, a remarkable endocrinologist who has the largest diabetes reversal program in Dubai and Lebanon, about this case. Even he thought it would be tough, but he’d reversed cases like this, so we gave it a shot.
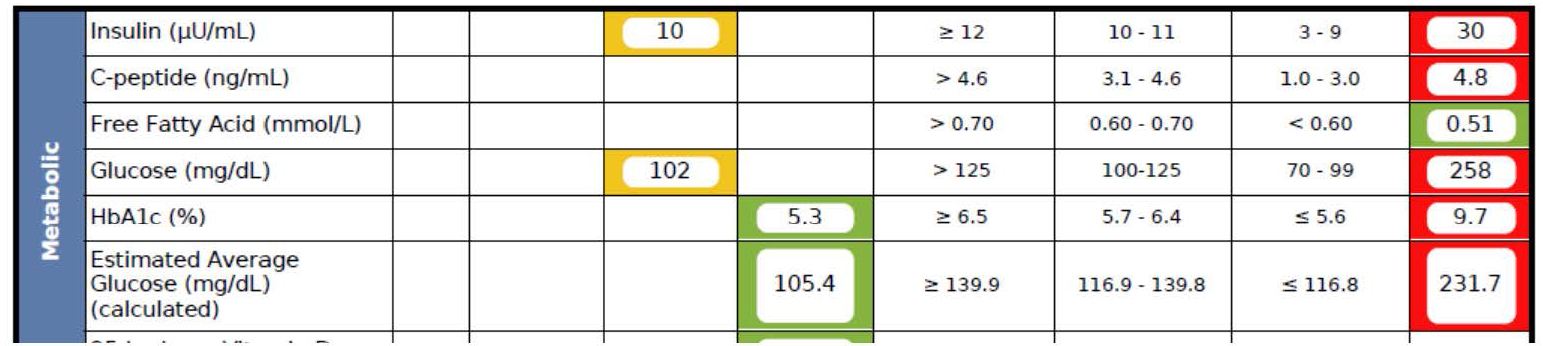
What happened over the next 5 months surprised me, as even I did not anticipate the alacrity of RB’s reversal. Below is a snap shot of RB’s labs from March 1, 2016 about 5 months after the OGTT, above. On the right side you can see the results from September 28, 2015, including the HbA1C of 9.7%, the fasting glucose of 258 mg/dL, and the fasting insulin of 30 uU/mL (HOMA-IR calculated at 19.1).
As you can see, the HbA1C fell to 5.3%—that’s even below the threshold of pre-diabetes—and the fasting glucose and insulin fell to 102 and 10, respectively (HOMA-IR calculated at 2.5).
RB doesn’t have diabetes any more. RB will avoid the amputations that destroyed the lives of his family. RB will not die prematurely from heart disease in his 50s. RB got a new lease on life.

If you think I’m telling you this story to impress you, you’re mistaken. Countless doctors (though not enough) know how to do what I did with RB—it’s actually simple biochemistry, and if a former surgeon like me can learn it, certainly anyone can, as long as one has the ability to frequently and safely manage medications and guide necessary behavior change. But sadly, most people like RB don’t have this option, and even if I and countless other doctors devoted the rest of our lives to helping everyone like RB out there, we could not put a dent in this problem, which is where Virta Health comes in.
Disclosure: I am an advisor to Virta Health and I have invested in the company, because I believe their approach is the best one to solve this problem—not the other way around.
Is it possible to deliver systematic diabetes reversal results (like the case above) safely, sustainably, and at scale among average diabetics?
Of course, even with the correct biochemical/nutritional approach, there are number of challenges to make T2D reversal possible at scale:
- Eliminating diabetes medications safely requires day-to-day (not monthly) careful adjustments by a physician. This is not how physicians work and would not be cost-efficient.
- Anything nutrition related requires a very high degree of individualization based on health status, lifestyle preferences and other life circumstances. For the 1% DIY’ers (who probably disproportionally read blogs like this one) any extreme approach can work, but at a population level, it won’t be enough.
- Both the patient and physician would need near real-time biomarker (e.g., CGM) data to adjust meds and the overall intervention. [By the way, I get asked all the time—mostly on Twitter—what CGM is…for those about to ask, here you go.]
- All behavior change and lifestyle interventions have failed at scale because only a small fraction of the population is able to DIY through complex decisions in today’s environment and life circumstances. This would require a near real time “personal coach” who can address any situation (e.g., family struggle, travel, new job, holidays).
It appears that we may be a step closer to somebody solving this challenge. Today, the first results of a T2D reversal clinical trial were published in the Journal of Medical Internet Research that show a promising new way to look at T2D: it is reversible in a large percentage of average patients, safely and sustainably. The trial was conducted by Virta Health, an online diabetes reversal clinic, which uses technology and artificial intelligence to solve the above mentioned care delivery challenges. The entire intervention is managed by physicians and the nutritional approach is based on highly individualized carbohydrate restriction and nutritional ketosis (which I’ve written about extensively in the past and throughout this blog).
The trial took place in Lafayette, IN, in partnership with Indiana University Health. A total of 262 women and men with T2D enrolled in the Virta Clinic. Average age was 54 (Stdev: 8); BMI 40.8 (Stdev: 8.9) and two-thirds of the patients were female. The trial will continue for at least two years, and data from the first 70 days were published today.
After just ten weeks:
- 56% of the diabetics enrolled achieved an HbA1C below the diabetic range (6.5%), while eliminating hypoglycemic medications
- Almost 90% of insulin users had it either completely eliminated (close to 40%) or reduced
- Mean body mass reduction was just over 7%, which is quite significant, but also shows that diabetes can be reversed before massive weight loss (i.e., it’s not the obesity that causes type 2 diabetes, which is consistent with the gastric bypass literature)
- Patient completion rate was >90%, which is remarkably high in an outpatient-based intervention.
- Reported feelings of hunger decreased from the pre-trial level (this seems to be a strong indication that will-power driven caloric restriction was not a factor in weight loss)
- Importantly, there were no serious adverse events, no incidence of symptomatic hypoglycemia, and no incidents of ketoacidosis.
The trial is ongoing with one-year data expected to be published shortly.
Yes, this is only one clinical trial and 70 days is not very long, but these data force us to consider that there is another way to look at T2D: it is not a chronic condition that gets progressively worse. With the combination of the right science and technology, it can be reversed at scale and among average diabetics. Clearly we need to look at the long-term success, and see many more patients succeed safely, but this is more promising than anything I have ever seen. I’ve seen some of the preliminary 1+ year analysis and the results look very impressive. I look forward to sharing them as they become publicly available.
If you are interested, you can learn more about Virta and their diabetes reversal science here. I’m excited to be a very small part of this organization and I look forward to the day when every patient with T2D at least has the chance to try an approach that can potentially reverse their condition.

Unrelated to current post but I have an elevated Lp(a) particle number. As you know it’s hereditary and my Mother and 1 of my 3 older Brothers have suffered a myocardial infarction. I’m in very good health (age 44) and have gone through a battery of stress tests, etc. and my doctors have finally told me to chill out. In Tim Ferris’ book you call it THE most atherogenic particle in the body. You go on to say we need to act on it indirectly as diet and drugs won’t do anything. What should I do? How do I “pull the lever harder on other things”?
In November 2015 I got the dreaded T2D diagnosis. A1C was over 9. My doctor put me on 1000mg of metformin and sent me on my way. He told me to come back in a couple of months for more tests.
I did not know anything about Keto diets at the time, but I had read the Atkins Diet book a couple of decades earlier and immediately went on a low carb diet. By my next appointment my A1C was down to 6.3 and I had lost about 25 pounds.
Since then I have learned a lot about Keto, and have been eating that way for over a year now. I have also incorporated intermittent fasting (5/2) and have done a few 3 day fasts. As of May 2017 my A1C is 5.5 and my LP-IR score is under 25 (the lab test did not have a specific number).
I like my doctor and am not trying to disparage him for not telling me anything about a low carb diet, I think he is just programmed to think that the response for most things is to prescribe a drug that the patient will blindly take for the rest of their lives. For instance, lately my cholesterol has gone up (although not everything in my NMR lipid profile is bad) and his first response was to try to get me on a statin. No discussion about other possible alternatives, or even if it is really a problem. I am not inclined to take one based on the research I am finding.
Hello Peter, I have been following your website and blog intermittently for a few years now. I recently watched a new documentary on Netflix called “What the Health”. I was wondering if you have had the chance to see this documentary yet and what you think. If you have not seen it yet I highly recommend it because it appears to be completely disagreeing with you. Also wondering if you have any paid sponsors for your website.
Dr. Attia,
I graduated with a bachelors in Nutrition and Food Science, then went to pharmacy school and
received my PharmD degree. I subsequently specialized further through 2 years
of residency training to become an ambulatory care clinical pharmacist. I first came across
your work from your TedTalk “What if we’re wrong about diabetes” while I was
preparing a CE presentation on diabetes and obesity. At that time I was in
my 2nd year of my pharmacy residency. It
made me question everything I had learned thus far in my career regarding
nutrition and diabetes.
It wasn’t until I encountered my “Patient 0” that I started to contrive and
implement the LCHF diet (through your inspiration and others like Sarah
Hallberg and Gary Taubes). That patient was my younger sister. She was 26
years old and just got a call from her doctor’s office saying her A1c was
5.8%, she has prediabetes. Although this number didn’t seem outrageous, I
was shocked. Yes, we have a family history of T2D, but we never thought a
diagnosis of prediabetes for one of my siblings could happen so soon. I
never considered my family unhealthy. We are Asian-american, with normal
builds, none of us would be considered overweight. Did I also mention, all
of my siblings are in the health field? (a pediatrician, 2 dentists, and me
the pharmacist). Surely, we knew what was “right” and “healthy”. But now we
were forced to question what we knew of conventional wisdom (ie. fat is bad) was wrong?
And so, I created a LCHF diet to test. The pilot subject was my sister. And you guessed it, it was successful! The next time she had her A1c rechecked it was 5.5%. No more prediabetes. Even though she was just 1 person, I knew it was worth trying to educate my prediabetic/diabetic
patients on this diet. I was starting to believe it was the “right”
one. Right off, I had dozens of patient’s lose weight, saw blood sugars becoming more regulated and their A1cs drop (ie. reversing their diabetes). What was also truly amazing from a pharmacist’s point of view was the need for LESS medications. I had numerous patients taken off/had reductions in their insulin, antihyperglycemics, blood pressure meds, etc.
Today I continue to stand by Hippocrates and his belief to “use food as thy
medicine, not medicine as thy food”. The LCHF diet has changed so many of my
patient’s lives and most importantly my sister’s and my family’s life for the
better. My newfound beliefs/practice has not gone without resistance from providers, peers, patients, etc., but I am determined to continue to advocate for what I think is best for my patients.
I wanted to thank you for being an inspiration to my clinical practice, for
reinvigorating my passion in nutrition and medicine in order to help others,
to question everything, and to continue our oath of life long learning in
order to provide the best care for our patients.
Hi Peter,
Have you watched the documentary, What the Health on Netflix? If so, what are your thoughts? It focuses on the message that high fat diets lead to diabetes, cancer, etc. instead of sugar and carbohydrates. I’m trying to do what’s best for my health but the conflicting information and opposing results from various studies is incredibly confusing.
Peter
This is terrific stuff. I haven’t visited your blog for a while so it’s great to see the new posts. I am an ophthalmologist who works in a clinic (and a country) bursting at the seams with obese patients with T2 diabetes. Our clinics are becoming overrun with patients requiring injections of VEGF into their eyes to control their retinopathy but the MDs and nutritionists seem resolutely stuck on their old models of care despite all the evidence for the benefits of carb reduction in T2D. I hope that eventually the message of your research and that of others will sink in but I’m not holding my breath. In the meantime I will refer my overweight patients to your site. Keep up the good work!
Impressive results. Congratulations to the team at Virta Health! If after two years and the results continue to be impressive (as I expect they will based upon my past 2.5 years in ketosis), do you have a guestimate of the percentage of doctors that will remain concerned about perceived dangers of long term (e.g., decades) ketosis?
I don’t know if anyone has tried this, but there appears to be a group of people that can reveal the long term safety of ketosis. People with drug resistant epilepsy are more or less forced to stay in ketosis in order to control their seizures. A retrospective study on this group of people could easily (and relatively cheaply) go back decades to determine how the prevalence of chronic disease changes over their time in ketosis,
There seems to be plenty of candidates for a study like this. There are about 120,000 adults in the U.S. with drug resistant epilepsy, a number based upon epilepsy prevalence estimates (see https://www.ncbi.nlm.nih.gov/pubmed/15331945) that about 0.5% of the U.S. population has epilepsy and 10% of those cases are drug resistant. (Concretely, 120,000 is roughly equal to 320,000,000 Americans * 0.76 adults/American * 0.005 prevalence of general cases of epilepsy * 0.1 proportion of drug resistant epilepsy among general cases of epilepsy.)
Best regards,
Greg
I like!
Great success!
jagshemash
Interesting article. What do you think?
https://time.com/5183350/diabetes-five-types/
Hi Peter,
I know you read about nutrition a great deal, so I wonder if you have thoroughly looked at the research supporting the efficacy of a “whole food, plant based” diet, for all sorts of health benefits including reversing diabetes? It seems to be the opposite of the low carb diet you write about so well. I wonder if you would ever be willing to do a “self experiment” of sorts, and perhaps compare your stats on your usual low carb diet to those you achieve after, say, 2-3 months on a true WFPB diet (with no added oils, minimal fat, no added sugars, etc). I’m speaking of the kind written about in the book by Neal Barnard, M.D. in “Dr. Neal Barnard’s Program for Reversing Diabetes: The Scientifically Proven System for Reversing Diabetes Without Drugs
by Neal Barnard | Feb 27, 2018”. Also, check out the many “Success Stories” on the ForksOverKnives.com website. I personally tried both low carb (under 50 g/day) and this WFPB diet, and had dramatically better results on the latter diet. I was truly not expecting that! The two diets do seem like polar opposites. In the interest of keeping an open mind, I would welcome your willingness to at least try the WFPB diet yourself. Of course, review the research (e.g., on https://www.pcrm.org/ , or any of the books by caldwell esselstyn, dean ornish’s book “The Spectrum”, etc), but really please consider trying it before you render judgment. Perhaps you will be as shocked as I was to find such a polar opposite diet is actually more effective for weight loss/control and lowering A1C levels. By the way, while I welcome your email reply if you have time, I don’t mean to start a contrarian post on your blog. My comments here are meant only as a suggestion for you, personally. I have enjoyed your passion for health and desire to really look at the data on nutritional matters. That is why I wanted to share this with you. Best wishes to you and your family. Laura
Here’s a succinct summary: https://www.pcrm.org/health-topics/diabetes
Totally Reversable !
In 3 months , A1C 7.2 down to 5.6 …reversed T2D based on LCHF or keto type diet and IF. Reduced my waist 36inch to 32, down 30lb in weight. Back to my Teenage weight. I am 62 now.
I would like to share my story … I had been what is defined as prediabetic for close to 9 years… Now I am 49. Typical fasting values would hover around 115 -120 and PP especially when on rice staple would exceed 200… Never took medicine … but I was increasingly aware that I would move to the next stage… Until one day in Feb-19 this year I just could not bear to look myself in the mirror and the shape I was in . My face had fat my belly though not excatly pot but was far from flat. I decided then to lose weight… I became a follower at diebetes.co.uk and read about visceral fat and hip size being the mother of all ills. Started by increasing the percentage of vegetables and decreasing the percentage of carb in my diet and essentially ate only twice a day once in the morning and once at supper / dinner time. Period in between were for tea , light biscuits etc…. I added brisk walking cross training and yoga as I knew that weight loss would have to be backed up with muscle frame to avoid a hollow look after weight loss. The first month was the most impressive and my HBA1c came down to 6.3 from a high of 7.5 . I got such a hang of weight loss and what I eat that I now started predicting the next day morning weight as I had started registering every morning weight under the same conditions of clothes and toilet habits. This continued till I lost about 10% of my body weight from 83 to 76 Kgs… Now in Jul-19 something magical happened…. As though a switch got operated my PP is around 100-105 no matter what I eat and fasting is 75-80… I feel my body returned to my 20’s … I feel my beta cells are back with a bang…. I now seek further advice on how to maintain such magical moments throughout life and save our bodies from the various abuse which we knowingly or unknowingly subject it to.
There are many angles coming at me but my toes feel perfect at low glucose levels ( A1c ). I was already low body fat. LCHF got my toe pain away, sure LCHF May be dangerous but so is the inability to walk.
sorry if this was addressed already in other comments, but I would like a better understanding of what “reversal” means in this context. I understand that patients have normal biomarkers such as glucose, HbA1c, insulin, etc, but the question is, does this require maintaining a low carb/keto diet for the rest of their lifes? Or any exposure to carbohydrates will bring back the diabetes? In other words, are there any markers for beta-cell function that were assesed? Is beta-cell function completely restored in these patients or are the biomarkers maintained within normal ranges simply by avoiding carbs exposure? thank you
This is a great question. Dr. Atria could you please answer this?
In looking at Dr. hallberg’s you tube video tedx at Perdue I believe she says mentions that exceeding your carb tolerance will cause it to come back. See her video. I am NOT a medical professional so I may be totally wrong in my interpretation of what she says.
Dr. Attia, thank you so much for seeing the “person” in the “patient.” I have Lupus (SLE) organ damage, hypoglobulinemia, only 67% lung capacity and Type 2 Diabetes thanks to the many steroids over the years. My Sugar goes up and down with the steroid doses. I remain on 10 mg prednisone daily with quarterly or more injection/infusions of steroids and often times more when I am very sick. Unfortunately, the steroids seem to be the best cure for most flare ups and major set backs. Would this program or your research be able to help in anyway with steroid induced type 2 diabetes? Thank you kindly for taking the time to read this.
I read with interest your article in the Kitsap County Medical Society Communique. Have you looked into the insulin increase with starvation? The first 2 weeks of starvation have rapid weight loss, but then insulin levels increase to slow the metabolism and preserve what it can, slowing the rate of starvation. It’s possible, if you’re correct that insulin resistance precedes obesity in some people, that the cell’s perceived insulin-glucagon ratio simulates this starvation state and makes the cells hold onto or even store energy inappropriately.